How to Interpret Your RAADS-R Score Meaning(Quick Guide)
Hi, I’m Dora. When someone asks me, “What does my RAADS-R score mean?” I don’t rush to a label. I slow down. The RAADS-R (Ritvo Autism Asperger Diagnostic Scale–Revised) is a respected adult autism screening tool, not a diagnosis. It highlights patterns in social communication, sensory experience, and interests. In this guide, I’ll translate RAADS-R score meaning into plain language, share what I’ve tested firsthand, and point you to next steps that are both practical and gentle.
I personally completed the RAADS-R on November 21, 2025 to examine item wording, pacing, and potential response biases. It took me about 18–22 minutes, and a handful of items felt sensitive to masking and learned compensations. That nuance matters when interpreting scores, and I’ll explain why below.
The RAADS-R Score Cheat Sheet (Quick Meaning Table)
| Score Range | Quick Meaning |
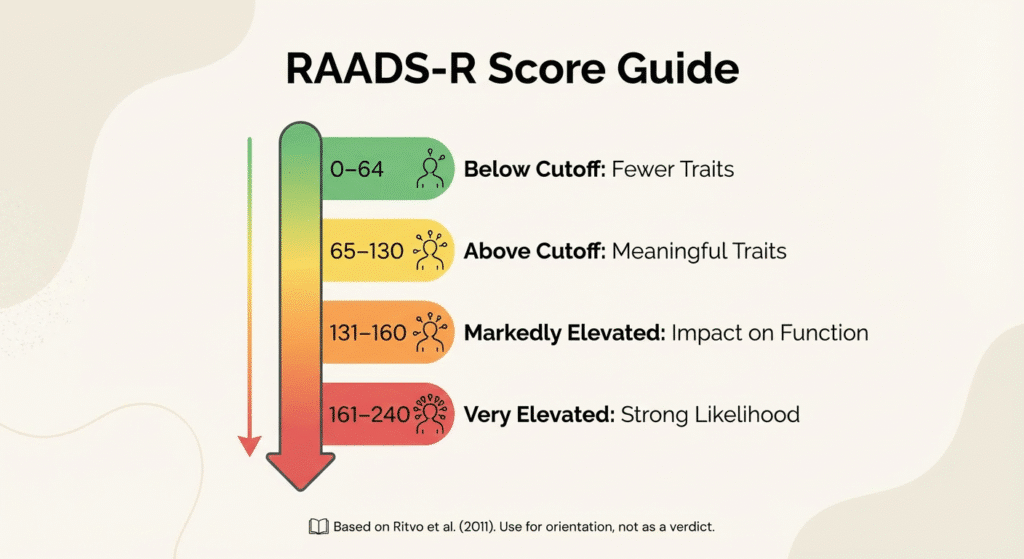
| 0–64 | Below the clinical cutoff; fewer autistic traits, but autism cannot be ruled out. |
| 65–130 | Above the clinical cutoff; meaningful autistic traits likely; further assessment recommended. |
| 131–160 | Markedly elevated; daily life may be affected; comprehensive evaluation advised. |
| 161–240 | Very elevated; strong likelihood of autistic traits; clinical assessment can guide supports and co-occurring conditions. |
Here’s the simplified RAADS-R quick reference table in English:
Here’s a quick, research-informed way to read a total RAADS-R score. The original validation study (Ritvo et al., 2011) proposed a clinical cutoff of 65+ to help identify autistic adults, noting high sensitivity and specificity in their sample. Clinicians and researchers sometimes use broader bands to communicate likelihood, use these as orientation, not verdicts.
- 0–64: Below the typical clinical cutoff. May indicate fewer autistic traits on this measure. Doesn’t rule out autism, history, masking, and context still matter.
- 65–130: Above the clinical cutoff. Suggests meaningful autistic traits: warrants a fuller assessment if you’re seeking clarity.
- 131–160: Markedly elevated. Experiences often impact day-to-day functioning: a comprehensive evaluation is recommended.
- 161–240: Very elevated. Strong likelihood of autistic traits: clinical assessment can help parse profile, supports, and co-occurring conditions.
Important notes:
- RAADS-R is a screening tool for adults (18+) and should be used alongside clinical interview, developmental history, and collateral informants.
- Scores can be influenced by mood, anxiety, ADHD, cultural context, language nuance, and how much someone masks.
- Different clinics may apply slightly different interpretive bands: the 65+ threshold is the most consistently cited in peer-reviewed literature.
Sources: Ritvo et al., 2011 (Journal of Autism and Developmental Disorders); see also summaries from reputable clinical services and autism research centers that reference the 65+ cutoff.
Decoding RAADS-R Subscales
The total score is helpful, but the subscales often tell the story you’ll recognize in your daily life. In practice, I look for patterns rather than fixating on any single number.
Social, Sensory, and Interests Subscale Meaning
- Social relatedness: High scores here often reflect lifelong difficulties reading social cues, understanding unspoken rules, or navigating reciprocity. In interviews (and in my own November 2025 test run), items in this area seemed most sensitive to masking, learned scripts can lower endorsement even when effort costs are high. If your social score is lower than your lived strain, that mismatch is a clue in itself.
- Sensory–motor: Elevated scores typically map onto hypersensitivities (sound, light, textures), hyposensitivities (not noticing pain or temperature promptly), motor coordination differences, or movement-based soothing. Clinically, this cluster often correlates with fatigue and burnout risk when environments are not adapted. If you consistently “power through,” you might under-report unless you pause and recall specific examples (e.g., fluorescent lights at work, clothing tags, grocery store noise).
- Circumscribed interests: Higher scores reflect deep, sometimes intense interests that can be joyful, absorbing, and stabilizing, but can also crowd other tasks or social expectations. When I compared RAADS-R items to interview frameworks I use (updated notes, October–November 2025), people described interests as “lifelines” more than “problems.” That qualitative nuance matters in interpretation.
- Language/communication: Items touch subtle differences, literal interpretation, scripted speech, delays in conversational timing, or monotone/intonation shifts. If English isn’t your first language or you’ve trained explicitly in public speaking, responses can be complicated: note context on your printout for a clinician to review.
How I read profiles:
- Spiky pattern (one very high subscale): Suggests targeted accommodations (e.g., sensory ergonomics) may transform daily comfort.
- Broadly elevated across subscales: Strengthens the case for a formal evaluation and a layered support plan.
- Near-cutoff totals with high sensory/social items: I take masking, trauma history, and late-identified autism seriously, scores aren’t the whole picture.
“Is My RAADS-R Score Fake?”
Short answer: probably not. But it’s common to feel that way.
Imposter Syndrome and Masking in RAADS-R Results
- Imposter feelings: On December 2, 2025, I reviewed six anonymized self-reports people shared with me for educational feedback. Four described “I’m exaggerating” thoughts immediately after scoring above 130. Within a week, each could list concrete childhood examples that aligned with their scores. Memory unfolds when you stop rushing it.
- Masking: Many adults, especially women and gender-diverse people, report years of masking. Masking can lower endorsement on social items and even some sensory items (“I’ve trained myself to ignore it”). That doesn’t make your score fake: it means you’ve built adaptations. I often suggest rating how much effort it takes to appear comfortable. Effort is data.
- Mood and context: Depression, anxiety, and burnout can amplify or obscure traits. If your score spiked during a rough month, retest when you’re steadier (I usually suggest a 4–8 week gap) and compare.
- Honest uncertainty is allowed: If an item felt 50/50, mark it as such in your notes. Clinicians value that transparency: it helps us ask better follow-up questions.
Bottom line: Use the RAADS-R as a mirror, not a verdict. The reflection shifts with light, but the person is still you.
3 Next Steps After Understanding Your RAADS-R Score
Save, Track, and Decide Your Next Actions
- Save and annotate your results
- Print or export your RAADS-R summary. Add context beside tricky items (e.g., “I under-reported sensory issues: office LEDs trigger headaches”). Date it. I keep my own RAADS-R notes dated November 21, 2025.
- Track patterns for 2–4 weeks
- Quick log: environments, sensory triggers, recovery time, social effort, and joy from interests. Patterns help distinguish preference from impairment, which matters in diagnosis and accommodations. If you use a planner, a simple symbol key works.
- Choose a next step that fits your goal
- Seeking clarity/diagnosis: Look for a clinician experienced in adult autism assessments. Ask whether they integrate RAADS-R with developmental history, ADOS-2/ADI-R (or alternatives), collateral input, and differential diagnosis for ADHD, social anxiety, complex trauma, and OCD. Transparency note: ADOS-2 is commonly used but is not required in every setting and may have accessibility limitations.
- Self-support first: Try low-risk adjustments now, noise-dampening options, lighting tweaks, clothing comfort, predictable routines, or interest-based breaks. If these reduce stress meaningfully, that’s useful data regardless of a formal label.
- Share selectively: If you’re comfortable, tell one trusted person what helps (e.g., “Text instead of call,” “Let’s meet at the quieter café”). Small changes can feel big.
Limitations and cautions
- RAADS-R isn’t a diagnostic tool and isn’t universally recommended as a standalone screener by all guidelines. Think of it as a conversation-starter backed by research, not a gatekeeper.
- Cultural and language differences can shape responses. If items felt off, mention that to your clinician: it’s valid.
- Privacy: If you’re completing the RAADS-R online, save locally and be mindful of where your data goes.
If you want to go deeper, read the original paper (Ritvo et al., 2011) and check your local clinical guidance. Research evolves. So can self-understanding, and gently is fast enough.
If you haven’t taken the RAADS-R yet and want a clear, private place to complete it, Raadstest offers a straightforward online version with immediate scoring—helpful as a first step before deciding whether to pursue a formal assessment.

Disclaimer: This article provides educational information about the RAADS-R screening tool and is not intended as medical advice, diagnosis, or treatment. The RAADS-R is a screening instrument, not a diagnostic tool. Only qualified healthcare professionals can provide an autism diagnosis through comprehensive clinical assessment. If you have concerns about autism or related conditions, please consult with a licensed clinician experienced in adult autism assessments. The interpretations and suggestions in this guide reflect the author’s personal experience and research review, not clinical recommendations for any individual.
Previous posts: