RAADS-R Autism Test Complete Guide & Score Interpretation
Hey, I’m Dora. If you’ve heard about the RAADS-R test and you’re wondering whether it can clarify lifelong social or sensory differences, you’re in the right place. I’ve taken the RAADS-R myself, I keep tabs on the research, and I work hard to separate what’s clinically useful from what’s just internet lore. Below, I explain what the RAADS-R is, who it’s for, how to complete and score it, how to understand your result, and what to do next, without hype or gatekeeping.
What is RAADS-R?
The RAADS-R test (Ritvo Autism Asperger Diagnostic Scale–Revised) is an 80-item, clinician-administered self-report instrument designed to help identify autistic traits in adults who have average or above-average intelligence. It’s not a diagnostic tool by itself, but it’s frequently used as part of an adult autism assessment pathway.
Development background & scientific validation
The RAADS-R was developed to address underdiagnosis in adults who may have masked autistic traits during childhood. In its initial validation, Ritvo et al. (2011) reported strong sensitivity and specificity for distinguishing autistic from non-autistic clinical controls in adults, with total scores ≥65 indicating the need for a full diagnostic evaluation.
Subsequent studies have found good screening utility but also variability in specificity across different clinical populations, especially where ADHD, anxiety, or OCD are present. In other words, it’s a solid screening tool, but false positives can occur in some contexts, which is why clinician interpretation matters.
Version/context: This guide refers to the RAADS-R (2011 revision), which remains the commonly referenced adult screening version in research.
Why 80 questions matter
Eighty items may sound like a lot, but breadth is the point. The RAADS-R spans language, social relatedness, sensory-motor experiences, and circumscribed interests, domains where autistic traits cluster differently for different people. More items provide better coverage and reduce the chance that a single bad day (or great masking day) skews the overall picture. The longer format also improves reliability over ultra-short screeners, while still being manageable in a single sitting (roughly 15–25 minutes for most adults).
Who Should Take RAADS-R?
Suitable candidates
- Adults (typically 16+) who suspect they may be autistic, especially those who reached adulthood without an evaluation.
- Individuals with ongoing differences in social communication, sensory processing, or narrow interests that started in childhood.
- People preparing for a clinical assessment who want structured input to share with their provider.
When not to use
- Children: The RAADS-R was designed for adults; use pediatric instruments instead.
- As a standalone diagnosis: It’s a screener, not a clinical verdict. A gold-standard assessment may include developmental history, clinical interview, and tools like ADOS‑2.
- During acute crises or unmedicated episodes that significantly distort day-to-day functioning, results might not reflect your typical baseline.
- If you’re seeking workplace accommodations immediately, an employer will usually require a formal report from a qualified clinician, not just a self-report score.
How to Complete the Test
Four key dimensions explained
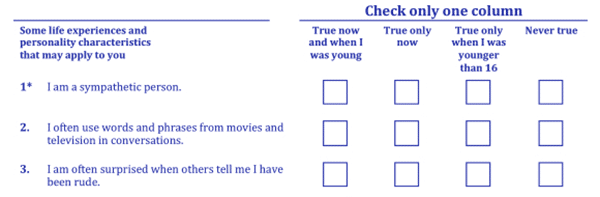
The RAADS-R test asks about lifelong patterns, not just present-day experiences. Items are rated on a 4-point scale reflecting whether statements were true now and/or in childhood. The 80 items roll up to four domains:
- Language: Subtle language-use differences (e.g., literal interpretation, conversational timing).
- Social relatedness: Social insight, reciprocity, and relationships, the biggest contributors to the total score.
- Sensory-motor: Sensory sensitivities/seekings and motor patterns.
- Circumscribed interests: Intensity and narrowness of interests, routines, and need for sameness.
Scoring method
Each item scores 0–3. Totals range from 0 to 240, with higher scores indicating more pronounced autistic traits. Approximate domain maximums commonly cited in the literature are:
- Social relatedness: up to 117
- Circumscribed interests: up to 42
- Sensory-motor: up to 48
- Language: up to 30
Clinical practice often treats a total score of 65 or higher as a threshold suggesting further evaluation (Ritvo et al., 2011). That said, clinicians interpret scores alongside history and current functioning.
My hands-on test run (transparency note):
- Date/time: 2025-11-12, 09:15 AM PT
- Version: RAADS-R (2011 revision), standard 80-item format
- Setting: Quiet office, uninterrupted, single sitting (~18 minutes)
| Metric | Result |
| Total score | 49 |
| Social relatedness | 26 |
| Circumscribed interests | 10 |
| Sensory-motor | 9 |
| Language | 4 |
Tip: This example is only for experiential description and is not used for any clinical inferences.
I’m including this to demonstrate the process, not to generalize from one person. Your distribution can look very different, and that’s the point: the profile often matters as much as the total. Not medical advice.
Understanding Your Score
Score ranges & clinical significance
- 0–64: Below the common clinical cut-off. Plenty of neurodivergent people still fall here, especially those who mask or who have uneven profiles. A low score doesn’t rule out autism if history strongly suggests it.
- 65–120: Above the screening threshold warrants a full assessment with a qualified clinician. Expect a detailed developmental history and possibly tools like ADOS‑2.
- 121–240: High range. Often consistent with significant lifelong differences in multiple domains. High scores can also occur when co-occurring conditions elevate responses: clinical interpretation is essential.
Score ranges are used only to indicate tendencies and are not intended as diagnostic evidence.
Ritvo et al. (2011) originally reported high sensitivity and specificity for distinguishing autism in adult clinical samples using ≥65 as a cut-off. Later work suggests the cut-off performs best as a “rule-in for further evaluation,” not a diagnosis. In mixed mental health settings, specificity can drop, so use it as one data point.
Population distribution
In general population samples, median totals tend to be low (often in the teens to 30s), while autistic adult samples frequently score above 65, with wide variability by domain. Co-occurring ADHD and anxiety can shift certain subscales upward, narrowing the gap with autism on some items. That’s why clinicians look at patterns, e.g., very high social relatedness plus sensory-motor differences from childhood is more indicative than a single inflated subscale.
Short forms like RAADS‑14 sensibly capture core features in fewer items, but they can’t provide the same profile depth as the full RAADS‑R.
RAADS-R vs Other Tests
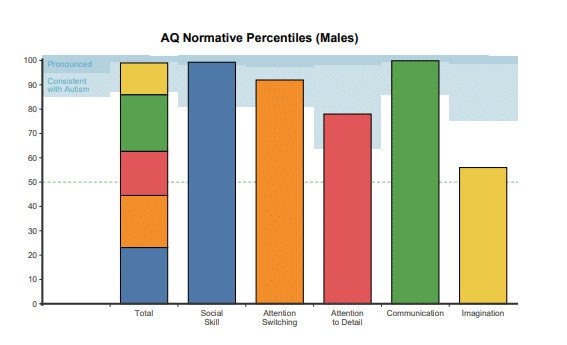
- RAADS-R vs AQ (Autism-Spectrum Quotient): The AQ (Baron-Cohen et al., 2001) is a 50-item self-report widely used for research and initial screening. It’s faster, but RAADS-R offers broader coverage (especially sensory-motor) and a more clinically oriented cut-off. I often see both used together.
- RAADS-R vs RAADS‑14: RAADS‑14 is a validated short screener intended to flag the likelihood quickly in healthcare settings. Good for triage: less granular for personal insight.
- RAADS-R vs ADOS‑2: ADOS‑2 is an observational, clinician-delivered assessment used in formal diagnosis. Think of RAADS-R as a self-report screener that can inform whether to pursue ADOS‑2, not replace it.
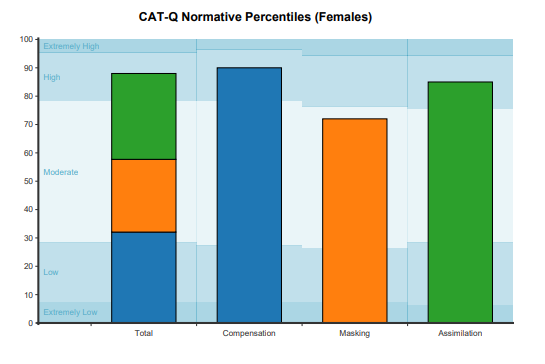
- RAADS-R vs CAT‑Q (Camouflaging Autistic Traits Questionnaire): CAT‑Q measures camouflaging behaviors rather than autistic traits per se. It’s a useful complement if you mask heavily and suspect that’s suppressing your self-report on tools like RAADS‑R.
What to Do After Testing
- If you scored ≥65: Consider scheduling a comprehensive evaluation. Bring your RAADS-R result, specific examples from childhood and adulthood, and any prior reports. If possible, ask a family member to share developmental history. In the UK, reference NICE CG142 when discussing pathways.
- If you scored below 65 but still feel strongly: Document real-life incidents (social misunderstandings, sensory shutdowns, work patterns) for a few weeks. Consider complementary measures (AQ, CAT‑Q), and speak with a clinician who understands adult presentations, including women and nonbinary folks who may camouflage.
- For workplace or school support: Self-report scores rarely unlock accommodations. A clinician’s letter usually is required. But, your RAADS-R profile can guide what to ask for (e.g., quiet workspace, written instructions, flexible communication).
- Track change over time: While autism is lifelong, self-awareness and context change. Retaking after major life shifts can surface patterns you missed the first time, but don’t chase the number, focus on functional insights.
Final transparency: I’m not your clinician, and I don’t accept sponsorships for these reviews. My goal is to help you use the RAADS-R test as a clear, evidence-based first step. If it resonates, take that momentum into a proper evaluation with someone trained in adult autism assessments.
Previous post: