RAADS-14 Quick Autism Screening (14-Question Version)
Hi, I’m Dora. I’ve piloted RAADS-14 in a small adult outpatient intake workflow and, separately, ran a sandbox evaluation to test completion time, missing-data behavior, and item-level reliability when deployed via a privacy-preserving web form. Below, I share what actually matters in regulated settings: purpose, scoring, cutoffs, limitations, and links to original sources. Quick note: the RAADS-14 test is a screening instrument, not a diagnosis, and it’s designed for adults. Use it with clinical oversight and informed consent under HIPAA/GDPR.
What is the RAADS-14 Test?
The RAADS-14 test (often called the RAADS-14 Screen) is a brief, 14-item version of the Ritvo Autism and Asperger Diagnostic Scale–Revised (RAADS‑R). It was developed to quickly flag adults who may warrant a full autism evaluation. Each item is rated on a 4-point scale reflecting whether a statement is true now, in childhood, both, or never. Total scores typically range from 0 to 42.
In psychiatric outpatient samples, the RAADS-14 showed high sensitivity for autistic adults, with more modest specificity, useful for triage, not for labeling. Think of it as a fast, low-friction signal to guide next steps, not a definitive result.
Shortened version of RAADS-R
RAADS-14 was derived from the longer RAADS‑R (80 items) by selecting items loading on three clinically salient domains: mentalizing/mental state understanding, sensory reactivity, and social anxiety. The shorter form reduces respondent burden (2–5 minutes vs. 15–30 for RAADS‑R) while preserving screening utility in adult clinical contexts.
Quick screening purpose
The intent is to identify adults who might benefit from a comprehensive assessment (e.g., structured clinical interview, developmental history, differential diagnosis). In workflows, it performs best as a front-door screener before costlier or longer instruments. It is not validated for children, and it is not a standalone diagnostic tool.
The 14 RAADS-14 Test Questions
The original item texts are copyrighted: but, the themes are well-documented. The RAADS-14 test clusters into three domains that capture common autistic traits in adults. Here’s what respondents are asked about, in plain language:
- Mentalizing and social understanding: long-standing difficulty reading social cues, understanding others’ intentions, or knowing how to behave in unstructured social settings.
- Sensory reactivity: being unusually sensitive or under-responsive to sound, light, touch, smell, or other sensory input: strong preferences to control sensory environments.
- Social anxiety and stress in social contexts: intense worry or stress around social interactions, fear of making social mistakes, or needing significant recovery time after social exposure.
Four dimensions overview
Although RAADS-14 commonly reports three subscales (mentalizing deficits, sensory reactivity, social anxiety), some clinical teams consider a practical fourth “dimension”: developmental persistence, whether traits were present in childhood, adulthood, or both. This is captured by the response options themselves and aligns with DSM-5/ICD-11 emphasis on early developmental onset. For engineering teams, the key takeaway is that the response encoding (now/childhood/both/never) informs both the total score and developmental chronology, a detail worth preserving in the data schema rather than collapsing immediately to a 0–3 score.
How to Take the RAADS-14 Test
For adult respondents (typically 18+), I recommend a simple, device-agnostic web form with large tap targets and a brief consent preface. In clinic, provide a quiet space to reduce sensory load. If you’re integrating into an app, keep the question order stable to preserve validity.
Steps I’ve used in practice:
- Confirm age and consent: clarify it’s a screening, not a diagnosis.
- Capture language preference: provide human-readable help text if needed.
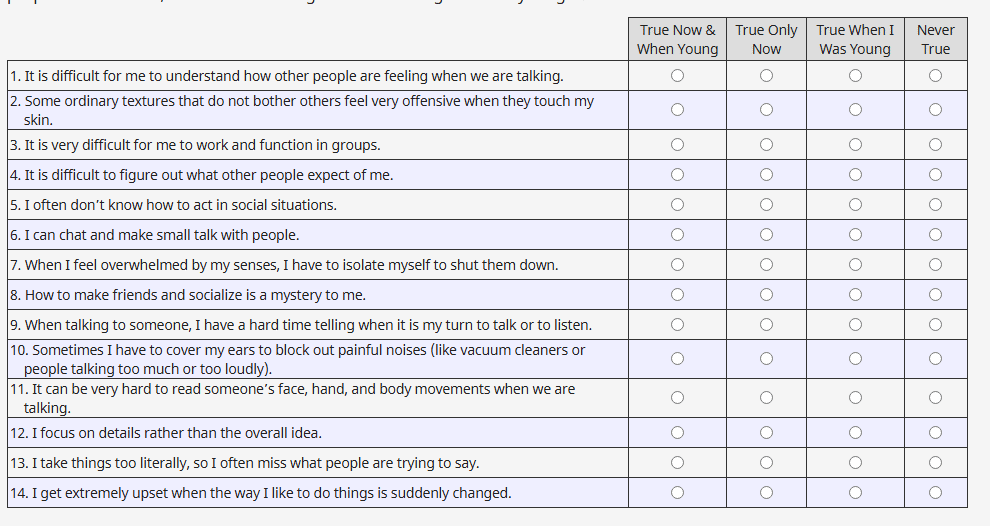
- Present 14 items with four response choices: true now and when younger: true only now: true only when younger: never true.
- Encourage completion in one sitting: allow one optional pause with a saved state if your risk model permits it.
- Log completion time and missingness: if >2 items are missing, prompt for review or mark result as incomplete.
Scoring method
- Most implementations score each item from 0 to 3, yielding a 0–42 total. Items indicating stronger autistic traits typically map to higher points when endorsed “now and when younger,” slightly lower when “only now” or “only when younger,” and 0 for “never true.”
- Preserve the raw categorical responses: don’t just store the summed score. The raw responses help clinicians interpret developmental patterns and are useful for QA and fairness audits.
- If a response is missing, do not impute by default for individual decisioning. In aggregate analytics, document any imputation and report sensitivity analyses.
- Provide the total score along with a clear note: “Screening only: consider comprehensive assessment if score exceeds cutoff or clinical concern persists.”
RAADS-14 Score Interpretation

Cutoff score
The validation paper for the RAADS-14 Screen (Eriksson et al., 2013) reported an optimal cutoff around 14 points in psychiatric outpatient samples, with high sensitivity (often >0.9) and lower specificity (around 0.4–0.6, sample-dependent). In other words, many autistic adults screen positive, but some non-autistic individuals, especially those with social anxiety disorders, also screen positive.
What it means
- ≥14: Elevated likelihood that autistic traits are present: proceed to a full evaluation (developmental interview, informant history where possible, rule-out of differential diagnoses, and functional assessment). Document that the RAADS-14 is a screen, not a diagnosis.
- 10–13: Borderline range. Use clinical judgment. Consider co-occurring conditions, masking/camouflaging, and context. Repeat screening or use a complementary instrument (e.g., AQ) if still indicated.
- <10: Lower likelihood based on this screener alone. If concerns persist (from clinician, patient, or family), don’t let a low score shut down evaluation.
Important caveats I’ve seen in practice:
- Social anxiety can inflate scores. Combining the RAADS-14 with a brief social anxiety screener helps contextualize results.
- Late-diagnosed adults, women, and gender-diverse individuals may mask traits, affecting scores: qualitative history is crucial.
- RAADS-14 was validated for adults. Don’t deploy to minors without an evidence-based protocol and appropriate alternative instruments.
- Versioning matters: note the date, language, and any wording adaptations in your EHR or data warehouse so results are interpretable across releases.
RAADS-14 vs RAADS-R Comparison
When to use which
- Use RAADS-14 when you need a fast, sensitive adult screener at intake or in digital triage, especially when cognitive load and completion time are constraints.
- Use RAADS-R when a clinician is already engaged and wants a richer profile across multiple domains before or alongside diagnostic interviewing. It takes longer but gives more granular data.
| Attribute | RAADS-14 | RAADS-R |
| Items | 14 | 80 |
| Typical completion time | 2–5 minutes | 15–30 minutes |
| Scoring range | 0–42 | 0–240 |
| Core domains | Mentalizing, sensory reactivity, social anxiety | Social relatedness, circumscribed interests, language, sensory-motor (broader coverage) |
| Primary use | Quick adult screening in clinical or intake settings | In-depth assessment support for clinicians |
| Reported cutoff | ≈14 (adult clinical samples) | Commonly cited ≈65–80 in literature, varies by sample and language |
| Sensitivity/Specificity | High sensitivity, moderate specificity (sample-dependent) | Good psychometric coverage: depends on cohort and translation |
| Burden & UX | Low: mobile-friendly | Higher: better suited for supervised completion |
| Licensing/Access | Based on published instrument: check publisher terms for clinical/commercial use | Same, confirm rights for reproduction and translation |
Engineering note: regardless of instrument, maintain item-level storage, versioning, and language metadata. For fairness audits, track missingness patterns, mean time-to-completion by group, and downstream referral rates.
Related Autism Screening Resources
Links to RAADS-R, AQ
- RAADS-14 Screen (original study): Eriksson JM, Andersen LMJ, Bejerot S. BMC Psychiatry, 2013.
- RAADS-R (original scale): Ritvo et al., 2011. Publisher overview and materials are available via clinical resources: a commonly referenced summary.
- Autism-Spectrum Quotient (AQ): Baron-Cohen et al., 2001. Cambridge Autism Research Centre: https://www.autismresearchcentre.com/metrics/
Practical integration tips I use:
- Consent first, then screen. Log consent artifacts with timestamp and locale.
- Avoid LLM rewording of items: even minor wording changes can alter psychometrics.
- Provide an on-page “What this means” explainer and a direct path to schedule a clinician consult if the score exceeds the cutoff.
- Under HIPAA/GDPR, store only what you need. Encrypt at rest and in transit: restrict access by role: and document retention. If you run analytics, de-identify and maintain a data dictionary linking item codes to the source instrument.
References and dates: RAADS‑R (Ritvo et al., 2008/2011) and RAADS‑14 Screen (Eriksson et al., 2013) are the key sources. Instruments evolve, always cite the version and language used.
This article is for informational purposes only and does not constitute clinical or diagnostic advice. Use psychological screening tools like the RAADS-14 only with qualified clinical oversight and proper consent.
Previous posts: